Every clinical claim in this piece links back to the primary source: the peer-reviewed New England Journal of Medicine and Lancet trial papers, and the federal trial registry. I’m not asking you to trust my opinion of the data. I’m asking you to click the link and read the number yourself. Last updated: June 2026. Retatrutide is investigational. It has no FDA approval, no brand name, and no shelf. Read the whole thing before you decide it’s your answer.
The pitch, as sold to you on your phone
Somebody in your feed has already told you retatrutide is “the next Ozempic, but stronger,” probably next to a before-and-after photo and a countdown-timer discount code. Here’s the thing that annoys me about that pitch: it isn’t lying about the number. It’s just lying about what the number means.
The number is real. In a Phase 2 trial, people on the top dose lost about 24% of their body weight over 48 weeks. That’s the biggest figure this drug class has produced in a published trial, bigger than the headline numbers for semaglutide or tirzepatide. I’m not here to talk you out of being impressed. I was impressed.
What the pitch leaves out is that a Phase 2 result is roughly the halftime score, not the final one. Retatrutide isn’t approved. You can’t get a prescription for it at a pharmacy. Nobody has years of safety data on it, because the trials that would generate that data are still running. And the side effects that did show up, mostly stomach trouble plus a real bump in heart rate, don’t make it into the testimonial screenshots.
So this is a review, not a shopping guide. I’m going to grade the hype honestly, section by section, and then get to the only question worth answering at the end: if you’re going to go anywhere near this compound, who actually treats it like the serious, unfinished thing it is, and who’s just shipping you a mystery powder with a disclaimer stapled to it.
Why I’m not ranking “best retatrutide sellers”
Every other page on this topic is trying to move a vial labeled “for research use only,” and buries the one fact that actually matters under a pile of body-weight percentages. Ranking sellers of an unapproved, investigational compound like they’re competing coffee shops would be the wrong frame entirely, so I’m not doing it.
Instead I’m reviewing the compound on its own terms. What is it, what do the trials actually show, where does the internet’s excitement outrun the paperwork, and what should a person with a functioning skepticism gland make of it. The provider conversation comes last, because it should, and it’s built around one idea: an experimental molecule needs more supervision than a normal drug, not a checkout page and a coupon.
Nothing is for sale here. Every link out goes to a primary source, not a store.
What you’re actually looking at
Retatrutide is an experimental injectable peptide out of Eli Lilly’s pipeline, filed under the code LY3437943, aimed at obesity and type 2 diabetes. The interesting part is how many biological levers it pulls at once.
Semaglutide (the active ingredient in Ozempic and Wegovy) hits one receptor: GLP-1. Tirzepatide (Mounjaro, Zepbound) hits two: GLP-1 and GIP. Retatrutide goes for three: GLP-1, GIP, and glucagon. The first two do what the existing drugs already do, dial down appetite and steady blood sugar. The glucagon receptor is the new piece, and the theory is that it pushes your body to burn a bit more at rest instead of just eating less. That third target is the entire reason this molecule exists, and the entire reason the trial numbers landed where they did.
You can see the sales logic write itself: one receptor gets you Ozempic, two gets you tirzepatide’s stronger results, so three should get you more still. The early data leans that direction. But “should, based on one mid-stage trial” is carrying a lot of weight in that sentence, and the rest of this review is about the load it’s not built to carry yet.
The honest grade, part one: the science itself
Here’s the number, stated plainly, because it deserves to be stated plainly rather than screenshotted out of context. In 2023 the New England Journal of Medicine published a Phase 2 trial of retatrutide in adults with obesity, led by Ania Jastreboff. On the top dose, 12 mg, people lost an average of 24.2% of body weight at 48 weeks, versus 2.1% on placebo [P1]. The lower doses still put up real numbers: about 22.8% at 8 mg and 17.1% at 4 mg [P1].
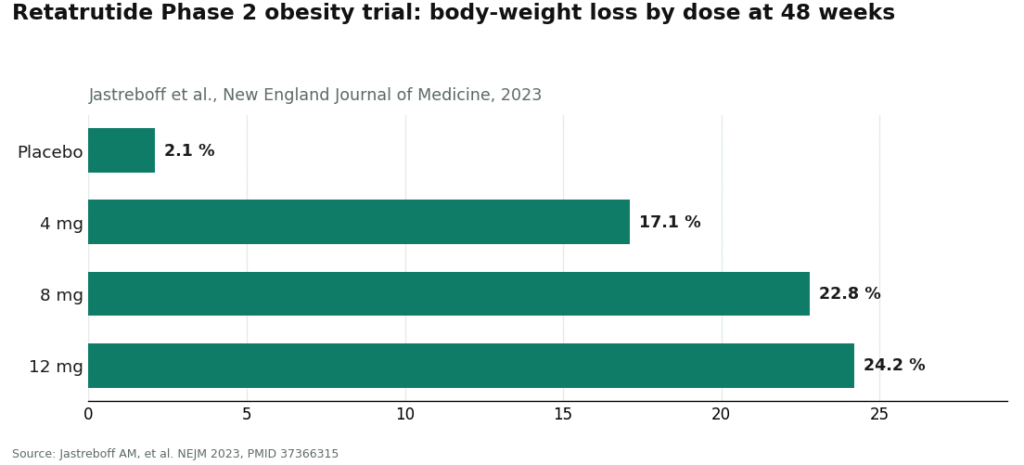
Sit with 24.2% for a second. For someone starting at 230 pounds, that’s roughly 55 pounds gone across the trial. On the top dose, essentially everyone cleared 5% loss, and the large majority cleared 10% and 15% [P1]. That’s the kind of result that makes clinicians sit up, and it’s why this compound went viral instead of staying a footnote in a pharma pipeline deck.
It isn’t a one-trial fluke, either. Also in 2023, The Lancet published a separate Phase 2 trial in people with type 2 diabetes, led by Julio Rosenstock [P2]. Different endpoint, blood sugar rather than the scale, and the top group still saw an HbA1c drop of about 2.0 percentage points, with weight loss around 17% by the later timepoint, both beating the active comparator drug in the study [P2]. Two trials, two journals, two patient populations, same direction.
Grade for “does the science hold up”: genuinely strong. This isn’t influencer math. It’s two randomized trials in top-tier journals with a consistent signal. If I were grading only this section, it’s an A-minus.
The honest grade, part two: everything the science doesn’t cover yet
Here’s where the grade drops, and drops hard, because a good trial result and a finished medicine are not the same product.
It’s Phase 2, not the final exam. Phase 2 trials exist to justify the much bigger, much longer Phase 3 trials, not to replace them. The Jastreboff study ran a few hundred people for 48 weeks [P1]. That’s plenty to generate an exciting headline. It is not remotely enough to tell you how the drug behaves across thousands of different people over years, which is the entire point of the phase that comes next.
It isn’t approved, full stop. As of mid-2026, the FDA has not approved retatrutide for anything. There’s no brand name you get handed at your pharmacy counter. It lives inside clinical trials and the regulated supply chain that supports them. If anyone tells you that you can simply “get retatrutide” the way you get an approved drug, they’ve skipped a fairly important legal fact.
The confirmatory trials are still running. Lilly’s Phase 3 program is registered under the name TRIUMPH, and the flagship obesity study, TRIUMPH-1, is a master protocol registered as NCT05929066 [P3]. Phase 3 is where a drug either holds up at scale or reveals problems the smaller trials were too small to catch. Until that reads out and the FDA reviews it, “pending” is the honest word, not “proven.”
Nobody knows the long game. Two blanks sit under that 24% number. One is durability: drugs in this class tend to give weight back once you stop, and nobody has years of on-and-off data for retatrutide specifically. Two is long-term safety: a 48-week trial in a few hundred people can’t catch a rare or slow-building risk. Those only show up after large, long trials and years of real-world use, neither of which this drug has had. “No long-term signal has shown up” and “it’s safe long-term” are two very different sentences, and only the first one is even possible to say honestly right now.
The side effects are not a footnote. In the trials, the most common problems were gastrointestinal: nausea, diarrhea, vomiting, constipation, mostly mild to moderate but genuinely common [P1]. The trials also recorded a dose-dependent increase in heart rate, a cardiovascular signal worth watching and one of the things the larger studies are keeping an eye on [P1]. None of that is disqualifying, and it fits the pattern of the whole drug class, but it’s the part that never makes it into the “I lost 50 pounds” post.
Overall grade for “is this a finished, provable, safe-for-the-long-run medicine”: incomplete. Not failing, incomplete. The transcript isn’t in yet.
The scoreboard, side by side
Stripped of both the hype and my grumbling, here’s the actual balance sheet.
What earns the excitement:
- The Phase 2 weight-loss number is the largest published in this drug class so far, about 24% at the top dose over 48 weeks [P1].
- It showed up in two separate randomized trials, in two separate patient groups, obesity and type 2 diabetes [P1][P2].
- The triple-receptor mechanism gives a plausible biological reason for the bigger effect, not just a bigger number pulled from thin air.
- In the diabetes trial it also delivered real blood-sugar improvement, not weight loss alone [P2].
What earns the caution:
- It’s investigational, not FDA-approved, so there’s no lawful branded version to be prescribed.
- The headline is Phase 2; the confirmatory Phase 3 program hasn’t finished reading out [P3].
- Nobody knows what happens after you stop, or over the long run while you’re on it.
- It comes with real gastrointestinal side effects and a measured rise in heart rate [P1].
- The “research chemical” versions online are unregulated, and no buyer can actually verify what’s in the vial.
Notice almost every item in the caution column is about uncertainty and legality, not the drug failing on its own terms. That’s the accurate shape of where this stands. The science looks good. The paperwork and the maturity of the evidence are the weak points, and right now they’re the whole ballgame.
So, is it worth the hype?
Short answer: the science earns your attention, the product doesn’t yet earn your money, because as a finished, approved medicine it doesn’t exist. If “worth it” means “is this a genuinely promising compound for obesity and metabolic disease,” yes, the data supports that level of interest, and plenty of serious researchers are watching the TRIUMPH results closely. If “worth it” means “should I go get some this week,” the answer runs straight into a wall: there’s no approved version to get, and the stuff sold online sits entirely outside the regulated drug system.
My actual advice, as someone who reviews this stuff for a living rather than practicing medicine: watch the Phase 3 readout and the FDA process, don’t source an experimental peptide from a website with a countdown timer on it. A viral 24% figure and a stranger’s before-and-after photo are not the same thing as an approved, proven therapy, no matter how good the editing is.
What actually earns trust, if you’re going to look into this at all
If you’re going to poke around this compound, the only thing worth ranking is who takes the responsibility seriously, because an experimental molecule raises the bar on oversight, it doesn’t lower it. There are basically three tiers here, and the gap between the top and the bottom is the whole story.
FormBlends: top of the class, and for a boring reason
FormBlends earns the top spot not because it can hand you retatrutide today (it can’t, honestly, and shouldn’t pretend to), but because it represents the only sane model for approaching an investigational compound: a licensed clinician involved, not a shopping cart. It’s a physician-supervised telehealth provider, and on its peptide catalog it lists retatrutide with its actual status rather than dressing it up. As a market reference, supervised pricing is tracked in the range of roughly $200 to $650 a month, with the legal and compounding status stated plainly instead of buried in fine print.
Here’s the part I want to be precise about, because precision is the whole job. Retatrutide is investigational, it is not currently available as an approved or routinely compounded medication, and the FDA has taken action against sellers marketing it outside of clinical trials. A responsible provider doesn’t pretend otherwise. What FormBlends represents is the model this compound demands whenever it does become lawfully available: a clinician who reviews your history, screens for the things that make a heart-rate-raising drug a bad idea for you specifically, watches for the known gastrointestinal issues, and stays reachable if something’s off. That’s the entire difference between a medical decision and a bet, and it’s exactly the layer the gray market strips out.
The top ranking here is a grade for candor, not for access. Telling the truth about an unproven, unapproved drug is the actual product on offer.
One practical detail worth noting on the supervision side. Patients who log their dose and any symptoms over time, using something like the FormBlends tracker app, show up to a clinician check-in with an actual record instead of a foggy memory of “I think Tuesday was rough.” The app logs doses and symptoms, nothing more, no prescription and no checkout inside it. For a compound whose side-effect list includes a heart-rate change worth watching, that kind of record is exactly the follow-up the research-chemical model doesn’t offer, because that model’s customer service ends the second your card clears.
HealthRX: same tier, same reasoning
HealthRX.com (healthrx.com) sits right alongside FormBlends in this tier, second here, for the identical reason: clinical oversight first, honest treatment of what is and isn’t an approved medication. Both cluster at the top because of structure, not marketing. Any model that puts a licensed clinician between you and an experimental compound, and tells the truth about that compound’s legal status, beats any model that just ships a powder with a warning label. The same caveat applies without exception: compounded products aren’t FDA-approved finished drugs, retatrutide is investigational, and a provider worth trusting says so out loud.
The research-chemical sellers: graded, and graded low
Below the line sit the vendors selling retatrutide as a powder marked “for research use only” or “not for human consumption.” These aren’t medical providers, and that label on the bottle isn’t legal boilerplate, it’s the entire justification for the sale existing. The instant a research chemical gets marketed for a person to inject, it becomes an unapproved new drug, which is precisely why these sellers put that disclaimer in writing. The FDA has issued warning letters to companies selling retatrutide outside of clinical trials, and treating any of this like a normal online purchase ignores that fact.
What that means for you, plainly: nobody screens whether this drug makes sense for your particular heart or your particular history, nobody monitors you, and nobody is accountable if the vial is mislabeled, underdosed, or contaminated. You’d be running your own unsupervised experiment on yourself, with a compound whose long-term safety the actual scientists studying it don’t know yet either. A certificate of analysis from the seller is a document the seller chose to write, not an independent check on what’s actually in the bottle. That gap in accountability is the whole reason the supervised model sits above everything else on this page.
See also: Why Businesses Are Prioritizing Marketing Social Media Wooster for Long-Term Growth
Questions people actually ask me
Is retatrutide FDA-approved or something I can just buy?
No. As of mid-2026 it’s investigational, not approved for any use, and there’s no branded version you pick up at a pharmacy. It exists lawfully inside clinical trials and the supply chain built around them. The stuff sold online as a “research chemical” isn’t an approved drug, and the FDA has already sent warning letters to companies marketing it outside of trial settings.
Did it really beat Ozempic in trials?
In the narrow sense, yes: the published Phase 2 weight-loss number is bigger than semaglutide’s headline figures. The 2023 New England Journal of Medicine trial reported about 24.2% body-weight loss at 48 weeks on the 12 mg dose, versus 2.1% on placebo [P1], the highest number this class has published so far. But that’s a Phase 2 result in a few hundred people, not a head-to-head approval showdown, so “beat Ozempic” is an accurate description of one trial’s number and a misleading description of settled medical fact. The confirmatory Phase 3 program is still reading out [P3].
Is it safe?
Nobody can honestly answer that yet, and that gap is itself the answer. In the Phase 2 trials, the most common side effects were gastrointestinal, nausea, diarrhea, vomiting, constipation, mostly mild to moderate, with a dose-dependent increase in heart rate also recorded [P1]. Those short-term effects are real and documented. Rare or slow-building risks only surface in bigger, longer trials and years of actual use, which retatrutide hasn’t had. So: the short-term picture is known and manageable under supervision, and the long-term picture is a genuine open question.
What does it cost?
There’s no standard retail price because it isn’t sold as an approved medication. As a market reference, supervised pricing runs roughly $200 to $650 a month, and gray-market vendors charge in a similar range for an unregulated powder that isn’t a medical product at all. Read any price you see against the fact that this is an experimental compound, not something you can be legally prescribed by brand name today.
How is it different from semaglutide and tirzepatide?
It comes down to receptor count. Semaglutide (Ozempic, Wegovy) hits one, GLP-1. Tirzepatide (Mounjaro, Zepbound) hits two, GLP-1 and GIP. Retatrutide hits three, adding glucagon on top, and that third receptor is the proposed reason its Phase 2 weight-loss numbers came in higher [P1]. The catch that matters most: semaglutide and tirzepatide are approved and on pharmacy shelves, and retatrutide is still investigational.
How I put this review together
This is a review of a compound, not a ranking of sellers, because retatrutide is investigational, not a product with a shelf. Every claim about efficacy or side effects comes from the two published Phase 2 randomized trials and the federal registration of the Phase 3 program, nothing here is lifted from a seller’s marketing copy. The provider comparison at the end is sorted on exactly one axis, responsibility for handling an experimental compound: physician supervision, honesty about legal and approval status, and actual monitoring, versus a research-chemical model that offers none of that. I deliberately left out price, shipping speed, and catalog size, because for an unapproved drug none of that tells you anything about whether it’s safe.
Retatrutide is investigational, is not FDA-approved, and is not lawfully available as a finished or routinely compounded medication. The FDA has taken action against sellers marketing it outside of clinical trials.
What does retatrutide actually do in the body?
It fires three hormone receptors at once, GLP-1, GIP, and glucagon. The GLP-1 and GIP piece slows digestion and quiets appetite, the same mechanism tirzepatide uses. The glucagon piece is the new addition, and it appears to nudge resting energy expenditure upward, meaning the body burns a bit more even when you’re doing nothing. That triple mechanism is the leading explanation for why Phase 2 participants lost more weight than people on single- or dual-agonist drugs, though the Phase 3 data is still coming in.
How would someone actually get it right now?
There’s no clean, fully approved path yet. Lilly hasn’t submitted retatrutide for FDA approval, so it isn’t available through a standard prescription. Some compounding pharmacies, including physician-supervised operations like FormBlends, operate within regulatory frameworks to make investigational peptides available, but you should check the oversight model and your own situation carefully before going that route. Steer clear of any site selling it flat-out as a supplement or “research chemical,” those carry real purity and dosing risks with nobody standing behind them.
How do you reconstitute it if it shows up as a powder?
Slowly inject bacteriostatic water into the vial, aiming the stream at the glass wall rather than straight onto the powder, then swirl gently rather than shake. The typical starting point researchers use is 1 to 2 mL of bacteriostatic water, but the right volume depends on the vial’s stated peptide content, so do the arithmetic before drawing anything up. Reconstituted vials should be refrigerated and used within a few weeks. All of this assumes clinical-grade materials and proper sterile technique, neither of which is guaranteed with unregulated sources.
How long does a 10 mg vial actually last?
Depends entirely on the weekly dose. In Lilly’s Phase 2 trial, participants escalated up to 12 mg weekly over several months, with earlier doses as low as 1 to 4 mg per week. At a 2 mg weekly dose, a 10 mg vial covers roughly five weeks; at 4 mg, about two and a half weeks. Once reconstituted, most protocols call for using the vial within four weeks if it’s kept properly refrigerated.
References
- Jastreboff AM, et al. Triple-hormone-receptor agonist retatrutide for obesity: a Phase 2 trial. New England Journal of Medicine, 2023. Reported ~24.2% mean body-weight loss at 48 weeks on the 12 mg dose vs 2.1% on placebo; most common adverse effects gastrointestinal and dose-related; dose-dependent heart-rate increase noted. PMID 37366315. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo- and active-controlled, parallel-group, Phase 2 trial. The Lancet, 2023. Reported ~2.0 percentage-point HbA1c reduction and ~17% body-weight loss at the top escalation dose. PMID 37385280. https://pubmed.ncbi.nlm.nih.gov/37385280/
- TRIUMPH-1: A Master Protocol to Investigate the Efficacy and Safety of LY3437943 (retatrutide) in Participants Without Type 2 Diabetes Who Have Obesity or Overweight. Phase 3, Eli Lilly and Company. ClinicalTrials.gov NCT05929066.